
Motivation and emotion/Book/2023/Indigenous Australian engagement in mental health services
What helps Indigenous Australians to engage with mental health services?
Overview
[edit | edit source]
Imagine ... Indigenous Australians all over Australia can access adequate mental health services. Doesn't seem too crazy, right? And, it is still something we are trying to work towards. In 2007, the National Indigenous Health Equality Campaign – now commonly known as the Close the Gap Campaign – was introduced by the Australian Government to achieve equality in life and health expectancy between Indigenous and non-Indigenous Australians. It is a well-known fact that the Australian Governments trajectory has fallen short and not succeeded in closing the health gap.
One major area that has not seen significant improvement since the launch of the campaign is the mental health and wellbeing of Indigenous Australians across Australia. [ I think it is important to define mental health for Indigenous Australians here. It is not the same as it is for White Australia. Indigenous Australian's mental health is closely tied to spiritual wellbeing and connection country] To address the issues facing Indigenous Australians in accessing these services, barriers and motivations need to be identified. Helping to remove these contingencies increases the likelihood of mental health services being accessed, and identifying motivators may allow services to tailor their approaches.
It is important to understand that services for Indigenous Australians must be just that, for Indigenous Australians. Many western approaches and theories may not be effective, and Psychologists may need to adapt these approaches to become more holistic in their entirety.
Some barriers that have been identified include poor access to mental health services (particularly in rural communities), bottleneck issues in Clinical Psychology as a whole is contributing to a lack of culturally appropriate services, social disadvantage, and racialisation within services. Motivators and enablers include the Aboriginal Community Controlled Health Services (ACCHS), and Tracy Westerman and Pat Dudgeon leading the way in Indigenous mental health research and development, and new generations of Indigenous Australians breaking the cycles of intergenerational trauma, with younger voices seeking services out. It is important to note that these motivators are both intrinsic and extrinsic motivational tools, allowing a greater impact for Indigenous Australian mental health services.
This book chapter discusses Indigenous Australian engagement in mental health services, specifically the barriers and motivators that are present in accessing these services. It also discusses why western psychological approaches are not always beneficial in Indigenous Health services, what other approaches can be used, and the individuals and organisations who are making headway for Indigenous Australian mental healthcare.
Relevant theories are highlighted throughout this chapter; The Framework for Aboriginal and Torres Strait Islander Peoples’ Mental Health and Social and Emotional Wellbeing, Self-Determination Theory, Health Belief Model, and Maslow’s Hierarchy of Needs and ERG Theory assist in highlighting this holistic concept of mental health.
 Focus questions:
|
Definitions
[edit | edit source]
What is motivation?
[edit | edit source]- Motivation is a complex internal state or external 'force' that enables individuals to engage in goal directed behaviour. It is the driver behind why individuals initiate, continue and end particular behaviour at a certain time. Motivational states aim to maximise rewards and reduce punishments.
Intrinsic and extrinsic motivation
[edit | edit source]- Extrinsic motivation can be defined as environmental reason to engage in a certain action or activity, this is often a requested behaviour that results in an extrinsic reward or consequence. Intrinsic behaviour on the other hand, is an internal force that drives an individual to engage in a certain action or activity. This drives comes from within, with external factors irrelevant to the decision to act or behave. As Intrinsic behaviour is internal drive, it is often driven by the desire to engage in one's personal interests and capabilities. Therefore, intrinsic motivation is the preferred motivator. Extrinsic behaviour has been shown to undermine an individuals quality of performance, autonomy, and is not helpful for long-term motivation. Intrinsic motivation allows the individual to place value on the action or activity, not driven by environmental factors.
Indigenous Australians
[edit | edit source]- Indigenous Australians are the people with familial heritage of those who lived on the Australian continent before British colonisation in 1788. Indigenous Australians have been the caretakers of the land for approximately 60,000 years. Since British colonisation, Indigenous Australians have experienced genocide, racial discrimination, and severe social, emotional, physical, and economical disadvantage. The effects of these events on Indigenous Australians is still evident today, with access to services such as mental health support severely lacking.
Decolonising psychological research
[edit | edit source]- For decades, psychological research has revolved around western practices, norms, and values often limiting its universality. While this research has made profound impacts in today's world, it is also culturally and spiritually limited. Many psychological theories revolve around the individual, and their needs and experiences. These theories can be difficult and often irrelevant to Indigenous Australians - especially those in rural and remote communities - as the importance of community, spirituality, connectedness, and nature are just as important. This holistic view of the world is often not applied in psychological theory. this calls for the importance of decolonising psychological research, and allow different cultural perspectives and values to be explored. This will broaden psychological approach, and allow further understanding and multicultural perspectives to be integrated into research. Dudgeon and Walker explain it is critical to decolonise psychological research and theories, while also demonstrating the need for wellbeing practitioners to utilise appropriate psychological theories to reduce ethnocentrism cultural racism by rejecting the mainstream methods and theories that solely revolve around western ideologies and practices. (Dudgeon and Walker, 2015).
The theories
[edit | edit source]
Maslow’s hierarchy of needs theory and ERG theory
[edit | edit source]- Maslow's hierarchy of needs is a psychological theory on what drives individuals behaviour and fulfilment. The pyramid has five sections, Maslow proposed individual's needed to successfully achieve in order to gain well-being. These sections are psychological needs, safety and security, love and belonging, self-esteem, and self actualisation. Maslow proposed the lower and larger levels of the pyramids represented the highest priority needs that were essential for survival. The higher levels allows us to achieve emotional well-being and fulfilment. As Maslow proposed this theory as hierarchical, the needs on the higher levels of the pyramid could not be achieved until those on the lower levels were met meaning some needs are more important than others (Caulton, 2012). Maslow argued that only after meeting all five needs, could humans achieve well-being and thrive in their environment. However it is important to note that Maslow himself did not use reliable sources or research methods when formulating his needs theory. One of the biggest criticisms of Maslow's theory, is that often needs are not hierarchical and need priority changes throughout life (Caulton, 2012). Alderfer's EGR model is a modern modification of Maslow's theory, and instead created three categories; existence, relatedness, and growth. Existence corresponds to psychological and safety needs, relatedness corresponds to social and self esteem needs, and growth corresponds to self-actualisation needs. ERG theory emphasises that these three categories are not hierarchical, and therefore an individual can be motivated by more than one need at a time, and will vary between individuals (Caulton, 2012).
National strategic framework for Aboriginal and Torres Strait Islander peoples’ mental health and social and emotional wellbeing
[edit | edit source]- The NIAA have developed a framework for Aboriginal and Torres Strait Islander people's mental health and social well-being. The framework highlights the intrinsic connection between mind, body, and the landscape (NIAA, 2017). The framework proposes to assist service providers in understanding; the mental health issues most commonly impacting Indigenous Australians, understand expected service delivery, guide the direction and ongoing development of mental health and well-being programs, guiding and supporting service providers to deliver adequate, culturally appropriate clinical services for Indigenous Australians, and support policy development and program implementation (NIAA, 2017). The NIAA proposes the use of the social and emotional well-being model, shown in Figure 1. This model highlights the connectedness and complex domains that support Indigenous people to have a strong and positive identity. It is important to note that this model is founded upon a collectivist culture, unlike many individualist psychological models. Culture is a critical component of mental health service delivery to Indigenous Australians. Indigenous Australian well-being involves a complexity of issues stemming from colonisation, grief, loss, cultural dislocation, trauma, abuse and violence has all resulted in intergenerational disadvantage. Because of these complexities, the social and emotional well-being model proposes seven overlapping domains that all revolve around the need for connectedness (NIAA, 2017).
Self-determination theory
[edit | edit source]- Self-determination theory explains individuals innate motivation to grow and change through three universal concepts. According to self-determination theory, individuals require the following to achieve growth; autonomy, competence, and relatedness (or connection) (Guardia, 2017). Self-determination theory highlights the importance that people feel in control of their own behaviour and goals, the desire to learn new competencies and acquire skills to succeed, and feel a sense of belonging to others around them (Guardia, 2017). Self-determination theory highlights the importance of intrinsic motivation and social interaction, which correlates with the social and emotional well-being model for Indigenous Australians.
Health belief model
[edit | edit source]- The Health belief model explains why individuals take a proactive approach to their health, and guides health promotion and disease prevention programs (Champion and Skinner, 2008). Our health beliefs influence our actual behaviour, and intrinsically motivate us to engage in proactive behaviours. The theory outlines five key factors that influence an individuals health behaviours;
- the individual’s perceived susceptibility to a condition.
- the perceived severity of having the condition.
- the perceived benefits of taking action.
- cues to action; the costs and other barriers in proactive health behaviours (psychological, monetary and physical).
- self-efficacy and confidence in ability to succeed (Champion and Skinner, 2008).
The Health belief model is a widely used tool in creating successful curriculums that can be implemented across communities. This model in conjunction with the social and emotional well-being model could assist service providers in developing culturally appropriate and effective mental health services. The Health belief model could also be modified to not only include the individuals perception of health, but the communities perception as well.
Barriers in accessing mental health services
[edit | edit source]There are still significant barriers for Indigenous Australians trying to access mental health services. While these are mostly exacerbated in rural and remote communities, Indigenous Australians residing in cities also experience disadvantage in accessing these services. These barriers are; limited or no access to culturally appropriate mental health services, bottleneck issues in clinical psychology as a whole, and social disadvantage.
- In 2019, two-thirds of Indigenous Adults reported low to moderate levels of psychological distress (66%) and 3 in 10 Indigenous Australians reported high or very high levels (31%) based on the Australia Bureau of Statistics findings.
- Suicide was the 5th leading cause of death among Indigenous Australians, compared to 14th for the whole of Australia. Of children aged 5-17, suicide was the leading cause of death in 2021.
- These statistics paint a grim picture for Indigenous mental health, and the task at hand to reduce these numbers and support Indigenous Australians to improve their social, emotional, and mental wellbeing (National Aboriginal and Torres Strait Islander Health Survey, 2018-19 financial year 2020).
With the assistance of the NIAA framework and needs models such as the Health belief model, social and emotional well-being model, and developing services that promote intrinsic motivation and community engagement, Indigenous mental health services can better cater to Indigenous needs.
Limited access to mental health services:
[edit | edit source]30-50% of rural and remote communities have no access to allied health services (Hunter, 2007). Many communities experience disadvantage here, and often when it is flagged with departments and the commonwealth, it is too late. While access to mental and allied health services is limited, culturally appropriate services are also not readily available. Traditional 'treatment' oriented approaches may not work here, as many Indigenous communities take on a communal approach (Hunter, 2007). The NIAA's social and emotional well-being framework should be used in treatment programs involving Indigenous Australians, presenting a collectivist and holistic approach. By increasing the possibility for these communities to access mental health services intrinsic motivation would increase, not just for the individual but the need for the communities overall well-being (Hunter, 2007). We cannot expect Indigenous Australians to be motivated to get help when they do not get access to services, or feel as though the services are not listening to their needs as a community. There is also very little research on effective preventative measures, and more work needs to be done to allow mental health service providers to visit these communities and listen to their specific needs, as each community may be different.
Bottleneck issues in clinical psychology:
[edit | edit source]It is a well known issue across Australia, that clinical psychology is lacking psychologists across the profession. Bottleneck issues stem from Universities limiting placements for undergraduate students to pursue Honours and Master's in Clinical Psychology due to funding issues. This has seen wait times for psychology appointments exacerbated, with many psychologists closing their books or having month long wait lists (Hunter, 2007). This has been even further exacerbated in rural and remote areas. If individuals in cities cannot get an appointment for months, rural and remote communities seem to be left without any support at all. On top of this crisis, a lack of culturally appropriate resources and service providers not being trained in cultural safety presents and even grimmer picture. Service providers need to be prepared before entering these communities to maximise trust and long-term changes, learning about different cultures, cultural safety and cultural competence. Rural students also struggle not getting enough funding, and find it easier to move to larger cities to pursue education. This leads them away from their own communities where instead this should be promoted. Allowing students adequate education in their own communities can encourage them to stay and assist their communities effectively, as they understand the norms, values, and ideologies they hold. If these communities have a service provider from their own area who understands their needs, motivation to access these services would improve greatly.
Social disadvantage:
[edit | edit source]Due to the intergenerational disadvantage experienced by Indigenous Australians, social disadvantage is a major barrier in accessing mental health services. Poor educational levels, household crowding, and financial strain all play a large part in why many Indigenous Australians do not reach out for help. Many Indigenous Australians are not educated on what mental health and well-being is, and ways to improve well-being. Some rural areas may not know that there are service providers that can assist in mental health and well-being. Poor education levels may also prevent individuals from accessing these services, as they themselves may not understand how they are feeling, why they are feeling that way, or how to express how they are feeling to another person. Household crowding places further strain on communities, with 14% of rural Indigenous Australians citing overcrowding as a stressor in their lives (Abbott et al, 2018). Overcrowding and financial strain place further stressors on the communities, and also limit their ability to access mental health services. With many remote indigenous Australians needing to travel to access services - cues to action in the health belief model - these costs outweigh the need to seek help, and these communities are often left to suffer in silence.
Motivators in accessing mental health services
[edit | edit source]Despite these barriers, there has been significant movement in the health services sphere with more people calling for service providers to receive more funding and reach these rural and remote communities, and provide culturally appropriate services to Indigenous Australians.
ACCHS:
[edit | edit source]The Aboriginal Community Controlled Health Services (ACCHS) is determined to provide more culturally appropriate services to Indigenous Australians and conduct more culturally relevant and appropriate research (Dudgeon et al., n.d). ACCHS providers are initiated by and based in local Indigenous communities, for Indigenous communities. Their goal is to deliver holistic and culturally appropriate services for Indigenous Australians. ACCHS has services in every state and endeavours to reach communities in need. Other mental health services should be in consultation with ACCHS to equip service providers with culturally appropriate care, so Indigenous Australians can feel confident that wherever they access mental health services, they will be seen, heard, and understood.
Motivated to break the cycle:
[edit | edit source]Many Indigenous Australians are working collectively and individually to break the cycles of intergenerational trauma, and disadvantage. Younger voices are seeking services to work through trauma and mental health issues. This intrinsic motivation demonstrates the need for culturally appropriate services, so individuals can follow through and receive treatment and in turn encourage others around them to take initiative. Supporting these Indigenous Australians will have a knock on effect as they support their communities and encourage others (Dudgeon et al, n.d). It is imperative for these services to understand self-determination is central to Indigenous health services. Due to racism and prejudice, many Australians have a misconception that Indigenous Australians do not want to help themselves, however it is simply due to the lack of availability to seek this help from services that understand the complexities and differences between general western ideologies and services and Indigenous tailored programs and treatments (Dudgeon et al, n.d).
Tracy Westerman and Pat Dudgeon:
[edit | edit source]Tracy Westerman and Pat Dudgeon are leading the way in Indigenous mental health. Western and Dudgeon are Indigenous Psychologists dedicating their careers to assisting Indigenous Australians access to appropriate mental health services, and developing programs and policies to assist services in providing culturally appropriate treatments (Westerman, 2004). Westerman and Dudgeon are offering new perspectives in Indigenous health services, highlighting both intrinsic and extrinsic motivations Indigenous Australians have in accessing mental health services. They have both been influential in decolonising psychological practice, breaking down differences between western approaches and Indigenous holistic beliefs and the importance of restructuring the approaches typically used psychological practice and theory (Westerman, 2004). Westerman and Dudgeon are giving a voice to Indigenous Australians and their right to access culturally appropriate services that meet their needs. The Dr Tracy Westerman Indigenous Psychology Scholarship Program, encourages Indigenous students to pursue a career in psychology. To date, the scholarship is supporting 41 Indigenous students who are in various stages of their degree. These students have access to mentors, tutors, networking, research and placement opportunities. This initiative allows Indigenous Australians to pursue a career that helps their own communities without the financial burden that is further strained through University fees (Westerman, 2004). Westerman and Dudgeon are advocating for Indigenous Australians across the country, and calling for all mental health services to be adequately equiped to address and understand the complexities of Indigenous mental health.
Graphs and case study
[edit | edit source]
![]() Ideally integrate this information into other sections
Ideally integrate this information into other sections
Graphs (Australian bureau of statistics)
[edit | edit source]- These graphs shed some light on the ongoing issues surrounding Indigenous Australians mental health conditions.
- Figure 2 represents Mental and Behavioural conditions by state/territory - people aged two years and over.
- Figure 3 represents most common mental and behavioural conditions, by sex - people aged two years and over.
- Both graphs have been cited from the Australian Bureau of Statistics.
-
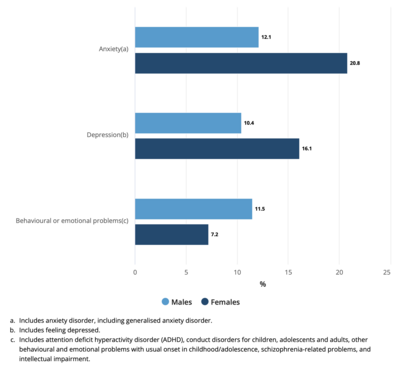 Figure 3: Most common mental and behavioural conditions, by sex - people aged two years and over
Figure 3: Most common mental and behavioural conditions, by sex - people aged two years and over -
 Figure 2: Mental and Behavioural conditions by state or territory - people aged two years and over
Figure 2: Mental and Behavioural conditions by state or territory - people aged two years and over


Case study
[edit | edit source]The below case study is a real life example of putting effective theory into practice. Although this case study does focus specifically on disease prevention, its framework and 8 stages of implementation are entirely relevant. Published by David Vicary and Henry Andrews in 2000.
A small Indigenous community in the north of Western Australia was experiencing multiple non-organic negative consequences as a result of FTT (failure to thrive). Specifically, many mothers in the community were young and due to their remoteness, had limited opportunities to learn nutritional and parenting skills for their children from their extended families (Vicary and Andrews, 2000). Elders in the community enlisted the assistance of non-Indigenous experts (the authors) to create such a service. Utilising their framework, which focuses on building relationships with Indigenous individuals, communities, and families, and building rapport - the authors created an 8 stage framework to ensure adequate services are delivered that are culturally appropriate and effective. These stages are:
By utilising these 8 steps, and focusing on the task as a community issue and not an individual issue, the service was a success as it met the communities cultural and community oriented approach. |
This case study demonstrates that through collaboration with Indigenous communities, and adjustments to a western approach taken in health service programs we can tailor mental health services to meet community needs while simultaneously targeting individual needs (Vicary and Andrews, 2000). Adopting a holistic approach is necessary in creating impactful change in Indigenous communities. through this approach, we rebuild trust with Indigenous communities and therefore will promote more intrinsic motivation. Through the health belief model, Indigenous Australians will seek out service providers to assist with their mental health as they see the positive changes occurring in their communities and see the effort service providers are going to in tailoring their approach to fit the needs of Indigenous Australians culture, identity, and connectedness to country and each other.
Quiz
[edit | edit source]Example simple quiz questions. Choose your answers and click "Submit":
Conclusion
[edit | edit source]We still have a long way to go to Close the Gap between Indigenous and non-Indigenous mental health service access, and we need to consider non western approaches to psychological theory in adopting a holistic approach that embeds Indigenous Australian beliefs and values. the health belief model and the social and emotional well-being model offer a starting point in addressing the gaps between western and Indigenous psychology perspectives. Indigenous Australians have a unique intrinsic connection between mind, body, landscape, and community. It is highly important to understand this in order to formulate appropriate models to motivate Indigenous Australians - both intrinsically and extrinsically - to access mental health services. By providing adequate health services to Indigenous Australians, intrinsic motivation will rise as they are given to opportunity to seek help.
- Theories
- The health belief model, and social and emotional well-being framework will help Indigenous Australians to engage in mental health services. If services better understand Indigenous needs, values, norms, and goals Indigenous Australians are more likely to engage and seek long-term help. Many Indigenous Australians face financial disadvantage, educational disadvantage and social isolation. By closing these gaps, motivation to seek out mental health services will increase, they simply need to be given the opportunity.
- Answers to focus questions
- Western psychological approaches are not always beneficial in Indigenous mental health services, as they present a western ideology and approach to mental health which does not correlate with Indigenous beliefs about mental health. Approaches must be tailored to these communities, or we will continue to see services that do not address these needs.
- The current barriers for Indigenous Australians accessing mental health services are the lack of services provided, the lack of culturally appropriate services being provided, and social isolation, financial strain, and intergenerational trauma. The multitude and complexity of barriers currently impeding Indigenous Australians from accessing services is vast and challenging, but highlights the importance of providing these services to begin with.
- Indigenous Australians are motivated to access mental health services to break the cycle of intergenerational trauma, and disadvantage. Indigenous Australians want to help themselves, and in turn help their communities to understand the importance of mental well-being. Closing the gap has been one of the biggest motivators of Indigenous Australians, and providing easily accessible services can assist in doing so.
- Pat Dudgeon and Tracy Westerman are leading the change in mental health services for Indigenous Australians, encouraging Indigenous students to pursue a career in psychology to help their own communities. Challenging what we know as psychologists and tailoring approaches that offer a holistic approach and are culturally competent.
- Take away message
- Changing psychological services is a long process and requires constant reflection, however it is imperative that Indigenous Australians are given a fair go at accessing services in order to improve their mental well-being. Intrinsic motivation is the main driver in engaging in mental health services, proving their willingness to engage and long-term gain that can be achieved. Intrinsically motivated individuals are more likely to engage in these services for longer periods of time, and will assist their own communities with mental health as it is not only the individual that matters. Holistic focus in these services is one of the most important changes that needs to be made.
See also
[edit | edit source]References
[edit | edit source]Australian Government. (2017, October 3). National strategic framework for Aboriginal and Torres Strait Islander Peoples’ Mental Health and social and emotional wellbeing 2017-2023. National Indigenous Australians Agency. https://www.niaa.gov.au/resource-centre/indigenous-affairs/national-strategic-framework-mental-health-social-emotional-wellbeing-2017-23
Caulton, J. R. (2012). The development and use of the theory of ERG: A literature review. Emerging Leadership Journeys, 5(1), 2-8.
Champion, V. L., & Skinner, C. S. (2008). The health belief model. Health behavior and health education: Theory, research, and practice, 4, 45-65.
Close the gap: Indigenous health campaign. The Australian Human Rights Commission. (1970, March 19). https://humanrights.gov.au/our-work/aboriginal-and-torres-strait-islander-social-justice/projects/close-gap-indigenous-health
Dudgeon, P., & Walker, R. (2015). Decolonising Australian psychology: Discourses, strategies, and Practice. Journal of Social and Political Psychology, 3(1), 276–297. https://doi.org/10.5964/jspp.v3i1.126
Dudgeon, P., Bray, A., & Walker, R. (2023). Embracing the emerging indigenous psychology of flourishing. Nature Reviews Psychology, 2(5), 259–260. https://doi.org/10.1038/s44159-023-00176-x
Dudgeon, P., Rickwood, D., Garvey, D., & Gridley, H. (n.d.). Working Together - Telethon Kids Institute. A History of Indigenous Psychology. https://www.telethonkids.org.au/globalassets/media/documents/aboriginal-health/working-together-second-edition/contents-and-introduction.pdf
Durey, A., & Thompson, S. C. (2012). Reducing the health disparities of Indigenous Australians: Time to change focus. BMC Health Services Research, 12(1). https://doi.org/10.1186/1472-6963-12-151
Guardia, J. G. L. (2017, February 26). Self-determination theory in practice: How to create an optimally supportive health care environment. Google Books. https://books.google.com/books/about/Self_Determination_Theory_in_Practice.html?id=bFF9AQAACAAJ
Hunter, E. (2007). Disadvantage and discontent: A review of issues relevant to the mental health of rural and remote Indigenous Australians. Australian Journal of Rural Health, 15(2), 88–93. https://doi.org/10.1111/j.1440-1584.2007.00869.x
Katz, I., Newton, B., Bates, S., & Ravon, M. (2016, March). Evaluation theories and approaches relevance for Aboriginal contexts. Aboriginal Affairs. https://www.aboriginalaffairs.nsw.gov.au/conversations/ochre/reports/Evaluation-theories-and-approaches-relevance-for-Aboriginal-contexts.pdf
Mental health. AIHW Indigenous MHSPC. (2023, May 15). https://www.indigenousmhspc.gov.au/topics/mental-health#aboutthistopic
National Aboriginal and Torres Strait Islander Health Survey, 2018-19 financial year. Australian Bureau of Statistics. (2020, May 26). https://www.abs.gov.au/statistics/people/aboriginal-and-torres-strait-islander-peoples/national-aboriginal-and-torres-strait-islander-health-survey/latest-release
Ryan, R. M., & Deci, E. L. (2000). Intrinsic and extrinsic motivations: Classic definitions and New Directions. Contemporary Educational Psychology, 25(1), 54–67. https://doi.org/10.1006/ceps.1999.1020
Vicary, D., & Andrews, H. (2000). Developing a culturally appropriate psychotherapeutic approach with Indigenous Australians. Australian Psychologist, 35(3), 181–185. https://doi.org/10.1080/00050060008257476
Vicary, D., & Bishop, B. (2005). Western psychotherapeutic practice: Engaging aboriginal people in culturally appropriate and respectful ways. Australian Psychologist, 40(1), 8–19. https://doi.org/10.1080/00050060512331317210
Vicary, D., & Westerman, T. (2004). That’s just the way he is’: Some implications of Aboriginal Mental Health Beliefs. Australian E-Journal for the Advancement of Mental Health, 3(3), 103–112. https://doi.org/10.5172/jamh.3.3.103
Westerman, T. (2004). Engagement of Indigenous clients in mental health services: What role do cultural differences play? Australian E-Journal for the Advancement of Mental Health, 3(3), 88–93. https://doi.org/10.5172/jamh.3.3.88
External links
[edit | edit source]Australian Bureau of Statistics: https://www.abs.gov.au/statistics/people/aboriginal-and-torres-strait-islander-peoples/national-aboriginal-and-torres-strait-islander-health-survey/latest-release#cite-window1
Modelling mental health service needs of Aboriginal and Torres Strait Islander peoples: a review of existing evidence and expert consensus (Page, Leitch, Gossip, Charlson, Comben, Diminic, 2022) https://doi.org/10.1111/1753-6405.13202
Tracy Westerman Scholarship Program: https://www.thejilyainstitute.com.au/about-the-scholarship/
Pat Dudgeon and Roz Walker: Decolonising Australian Psychology: https://jspp.psychopen.eu/index.php/jspp/article/view/4857/4857.pdf