
Motivation and emotion/Book/2016/Mental health help-seeking motivation
What motivates people to seek help and not seek help for mental health problems?
Overview
[edit | edit source]|
John and Peter both suffer from depression. One day John is reading an article in a magazine and comes across an article about depression. While reading through the article he decides to seek out help as he is experiencing many of the described symptoms. After a year of intensive treatment the severity of his depressive symptoms have reduced dramatically and John is looking forward to a brighter and happier future. Peter, on the other hand, suffers in silence for several years and while he knows something is not right he does not believe he needs help. His family and friends urge him to seek out treatment as they have noticed a drastic change in his overall demeanour but Peter still does not seek help. Over time, Peter plunges deeper and deeper into his depression, alienating everyone around him. Peter's wife decides to try and give him the motivation to seek out psychological help by telling Peter that she can no longer tolerate his moods and his refusal to seek help even though it is clear that he needs it. She moves out of the family home taking the children with her. Peter still does not seek help for his depression and instead tragically ends his life via suicide. |
Unfortunately, Peter's experience is not uncommon. The World Health Organisation estimates that as many as 25% of the world's population currently suffers from some kind of mental disorder and, of these people, only 30% of them seek out help, thus making mental illness one of the leading causes of disability and ill-health globally (World Health Organisation, 2001). Failing to treat mental disorders can lead to poor quality of life, social isolation (O'Connor, Martin, Weeks, & Ong, 2014) and major economic costs to the community (Whitefor, et al., 2014). Additionally, one of the most tragic consequence of not having a mental illness treated is suicide which accounts for approximately 785,700 deaths worldwide every year (O'Connor, Martin, Weeks, & Ong, 2014).
So why is it that John sought out help and Peter did not? This book chapter will outline what motivates people to seek or not seek help when they are suffering with a mental illness.
The key questions that will be answered in this chapter are:
- What psychological theories explain mental health help-seeking motivation?
- What barriers inhibit motivation for seeking out assistance with mental health issues?
- What strategies can be implemented to increase the number of people that seek out treatment for mental illness?
Australian Prevalence and Treatment Rates
[edit | edit source]In Australia the estimated prevalence rates and treatment percentages for mental disorders are slightly more promising than the global estimates and these figures are outlined in Table 1 and Table 2 (Whiteford, et al., 2014).
Table 1. Estimated prevalence and number of people with a mental disorder by age group
| Age Group | Prevalence | 2009-2010 |
|---|---|---|
| 0-15 years | 15.4% | 697,657 |
| 16-64 years | 22.2% | 3,282,449 |
| 65-74 years | 13.6% | 219,523 |
| 75+ years | 16.1% | 223,092 |
| Total | 20.1% | 4,422,721 |
Table 2. Estimated numbers of people with a current mental illness seen by mental health-specific services
| 2009-2010 | Percentage | |
|---|---|---|
| State and territory mental health services | 367,870 | 8.32% |
| MBS-funded mental health services (GP only) | 533,261 | 12.06% |
| MBS-funded mental health services not included
in the counts above |
833,519 | 18.85% |
| DVA mental health cares | 55,628 | 1.26% |
| Total | 1,790,278 | 40.49% |
Definitions
[edit | edit source]
Mental Disorder
[edit | edit source]A mental disorder is defined in the DSM-V (American Psychiatric Association, 2013, p. 20) as:
A mental disorder is a syndrome characterized by clinically significant disturbance in an individual's cognition, emotion, regulation, or behavior that reflects a dysfunction in the psychological, biological, or developmental processes underlying mental functioning. Mental disorders are usually associated with significant distress or disability in social, occupational, or other important activities. An expectable or culturally approved response to a common stressor or loss, such as the death of a loved one, is not a mental disorder. Socially deviant behavior (e.g., political, religious, or sexual) and conflicts that are primarily between the individual and society are not mental disorders unless the deviance or conflict results from a dysfunction in the individual, as described above.
Help-Seeking Behaviour
[edit | edit source]Help-seeking is defined as the following:
In the mental health context, help-seeking is an adaptive coping process that is the attempt to obtain external assistance with a mental health concern (Rickwood & Thomas, 2012, p. 180).
Traditional Masculinity Ideology
[edit | edit source]The term traditional masculinity ideology refers to the beliefs that some men have as to the importance of behaving in a way that matches with the perceived traditional societal norms of how men should behave (Levant et al., 2013). This ideology is measured using the Male Role Norms Inventory-Revised (MRNI-R) which proposes that there are seven traditional norms (avoidance of femininity, restrictive emotionality, self-reliance, dominance, toughness, non relational sexuality and negativity towards gay men) that men may feel they need to adhere to. Men who score low on the MRNI-R are more likely to have low self-esteem and self-efficacy (Levant et al., 2013).
Attitudes
[edit | edit source]Attitudes are the beliefs a person has about a specific behaviour and whether it has a positive or negative outcome (Roberto, Shafer, & Marmo, 2014).
Subjective Norms
[edit | edit source]Subjective norms are the beliefs a person has as to what they believe other people think they should do (Roberto, Shafer, & Marmo, 2014).
Perceived Behavioural Control
[edit | edit source]Perceived behavioural control refers to the belief a person has around the difficulty of carrying out a specific behaviour or action (Roberto, Shafer, & Marmo, 2014).
Stigma
[edit | edit source]Stigma is defined as the perception of being flawed because the individual does not conform to what is deemed to be socially acceptable (Vogel, Wade, & Haake, 2006). There are two types of stigma, public stigma and self-stigma (Vogel, Wade, & Haake, 2006). Public stigma is the views held by a group that specific behaviour exhibit by an individual is unacceptable and this group then acts negatively toward them (Vogel, Wade, & Haake, 2006). Self-stigma is when a person self labels their behaviour as socially unacceptable which then leads to a reduction in self-efficacy and self-esteem (Vogel, Wade, & Haake, 2006).
Help-Seeking Motivation Theories
[edit | edit source]There are a number of different psychological theories that have been proposed that can help explain mental health help-seeking motivation.
Health Belief Model (HBM)
[edit | edit source]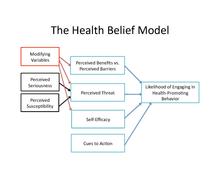
The health belief model proposes an explanation as to why individuals participate in positive and proactive health behaviours such as taking medication or seeking out professional assistance or eating healthy foods . O’Connor, Martin, Weeks and Ong (2014) outline the five factors that determine whether a person will participate in proactive health behaviours
- the individual’s perception on whether or not they are susceptible to the particular condition.
- the perception around the severity of the consequence as a result of having the condition.
- the perception around how beneficial the individual feels taking action would be.
- the costs and other barriers related to engaging in proactive health behaviours such as psychological, monetary and physical.
- the positive health values the individual has (O'Connor et al., 2014).
Theory of Reasoned Action and Planned Behaviour
[edit | edit source]The theory of reasoned action and planned behaviour posits that the best predictor of whether or not a person completes an action or behaviour is their intention to complete or not complete the behaviour (Roberto, Shafer, & Marmo, 2014). To predict a person's intention to act the theory of reasoned action and planned behaviour suggests that the person's attitudes, subjective norms and perceived behavioural control play a key role.
Specific to help-seeking behaviour, this theory proposes that help-seeking behaviour for a mental illness will occur when the individual overcomes belief barriers to seek help as a way to increase their expectations that treatment will have a positive outcome (Demyan & Anderson, 2012). This change in expectations will lead to an increase in positive attitudes, which in turn impacts in their intention thus leading to a behavioural outcome of sourcing treatment (Demyan & Anderson, 2012).
Social Cognitive Theory
[edit | edit source]According to social cognition theory is that personal behaviour, the environment and individual cognition interact with each other to determine how a person acts in different situations. The environmental situations that could impact the way in which a person behaves could be based on the family environment or the social environment (peers, race, the community as a whole) and whether these people agree with the action the individual is taking. Individual cognition could be defined in terms of self-efficacy for the purposes of this theory and if a person does not believe they have the personal competence to deal with a stressful situation then they are unlikely to be able to deal with these situations effectively (Levant, et al., 2013).
As an example to directly relate to help-seeking behaviour, if a person is in an environment where their family members do not believe that mental disorders exist or that professional assistance is required and the person does not believe they have the competence to seek help then they are unlikely to exhibit help-seeking behaviours.
Gender Role Strain Paradigm
[edit | edit source]The gender role strain paradigm proposes that Traditional Masculinity Ideology in a male’s culture causes him to act in accordance with these “guidelines” which leads to the male experiencing gender role strain (Levant et al., 2013). One of the most documented types of gender role strain is Gender Role Conflict, which is in reference to the conflict a man experiences when trying to conform to the ideologies of masculinity but also being in a situation that requires him to act against them (Levant et al., 2013). Both Traditional Masculinity Ideology and Gender Role Conflict have been found to be negatively associated with whether or not males will seek help for mental disorders (Levant et al., 2013).
Quiz
[edit | edit source]Take this quiz to review the theories behind help-seeking motivation.
Barriers to Help-Seeking
[edit | edit source]
Attitudes and Personal Characteristics
[edit | edit source]
Gender
[edit | edit source]
When it comes to seeking health for mental disorders, men are less likely than women to seek out help (Wendt & Shafer, 2016). Men are typically required to conform to masculine ideals that place importance on not showing personal weakness, self-reliance and not displaying emotions (Wendt & Shafer, 2016). When a man feels like he does not conform to these societal norms it lead to higher rates of suicide, substance abuse, conduct disorder, antisocial behaviour, sexual deviance and aggression in men when their mental health issues are left untreated (Levant et al., 2013).
Research has shown that when a male scores high in traditional masculinity ideology, they are more likely to have a high level of self-efficacy and self esteem so that they are able to overcome any self-stigma associated with seeking help (Levant et al., 2013). This supports the proposition of the social cognitive theory whereby a person who feels like they have the ability to handle stressful situations will be more motivated to seek help (Levant et al., 2013).
Ethnicity
[edit | edit source]Prevalence rates of mental disorders in both the Caucasian and African American populations are very similar, however African Americans are less likely to seek help from professional services than their Caucasian counterparts (Barksdale & Molock, 2008). Studies have shown that instead of approaching mental health professionals, African Americans are more likely to seek guidance from places such as clergy from their church, non-mental health professionals, family and friends (Barksdale & Molock, 2008). Research has suggested that this is because African Americans have additional significant barriers such as fears of being seen in a negative light by family and friends, fear of being institutionalised and cultural mistrust (Barksdale & Molock, 2008). Along with these barriers, African Americans have a tendency to be in denial about the severity of mental disorders and lean towards utilising strategies of self-reliance and determination to overcome their problems (Barksdale & Molock, 2008).
Most literature highlights the importance of family in the African American community (Barksdale & Molock, 2008). Whilst the additional barriers listed above all play a role in explaining why they do not seek professional help for mental disorders, family is the prominent factor in predicting a persons help-seeking behaviour which supports the theory of reasoned action and planned behaviour (Barksdale & Molock, 2008). Seeking help is generally not congruent with African American societal norms with many of the teachings within that culture promoting privacy and keeping family business in the family therefore directly contradicting the need for disclosure when seeking help (Barksdale & Molock, 2008). These negative attitudes from the family group is the prominent reason why African American people underutilise professional mental health services (Barksdale & Molock, 2008).
Age
[edit | edit source]Another barrier to why someone will not seek out professional help for a mental disorder is age. A person that is between the ages of 30 and 40 years is more likely to seek help for their mental disorder than those in younger or older age groups (Barksdale & Molock, 2008). In fact, those in the 16 to 24 year age group are more likely to experience a mental disorder than any other age group (Gulliver, Griffiths & Christensen, 2010). In Australia, the actual percentage of the 16 to 24 year age group seeking out professional mental health services drops to 25% from the overall percentage of 40.49% as listed in Table 1 (Gulliver, Griffiths & Christensen, 2010).
Studies have suggested that the reason why people in this age group are less likely to seek help revolve around a number of different reasons however the addition of low mental health literacy and a lack of emotional competence in the younger age groups seems to account for the decrease in help-seeking behaviour (Rickwood, Deane, & Wilson, 2007). Mental health literacy refers to the ability of a person to identify mental health problems, knowledge about the consequences of not seeking treatment and knowledge about where to seek treatment (Rickwood, Deane, & Wilson, 2007). Emotional competence refers to the ability to understand the emotions being felt and being able describe them effectively (Rickwood, Deane, & Wilson, 2007). This supports the theory of reasoned action and planned behaviour due to the fact that if a young person does not have the knowledge of where to get help or how to describe the issues they are facing, this could mean that they have a lack of perceived behavioural control and will be less motivated to seek out professional help.
Research has also shown that young people are less likely to be motivated to seek mental disorder help when they have low perceived benefits, high perceived barriers, low in extraversion and high in social support (O'Connor, Martin, Weeks, & Ong, 2014). These findings support the proposition of the health belief model that when perceived benefits of seeking out help outweigh perceived barriers to seeking help then a person is more likely to access mental health services (O'Connor, Martin, Weeks, & Ong, 2014).
Stigma
[edit | edit source]Stigma of oneself along with the stigma by the community as a whole regarding mental illness is one of the common barriers across gender, age and ethnicity (Vogel, Wade, & Haake, 2006). Studies have shown that in many cases that people who seek mental health assistance are often perceived in a negative way within the community (Vogel, Wade, & Haake, 2006). These perceptions make way for stereotyping, prejudice and discrimination towards help-seeking individuals (Vogel, Wade, & Haake, 2006). Some of the direct consequences of this type of public stigma is the increase of negative attitudes towards people needing assistance, a decrease in adherence to treatment, as well as a cessation of treatment altogether (Vogel, Wade, & Haake, 2006). Given the fact that public stigma increases negative attitudes towards help seeking behaviour, these findings support the theory of reasoned action and planned behaviour theory.
The self-stigmatisation of being inadequate or inferior because mental health assistance is required is another major factor in predicting if a person will display help-seeking behaviours (Vogel, Wade, & Haake, 2006). In the instance of a person experiencing high levels of self-stigma, they are less likely to seek help as it is a sign of weakness or they feel like they have failed (Vogel, Wade, & Haake, 2006). Self-stigma has been found to directly relate to a persons self-efficacy and self-esteem tying in closely with the social cognitive theory (Vogel, Wade, & Haake, 2006). When a person perceives that they lack competence to effectively gain assistance with their mental health issues then they are going to be less motivated to seek out professional help (Vogel, Wade, & Haake, 2006).
Strategies to Increase Help-Seeking Motivators
[edit | edit source]A significant factor in improving overall well-being for those suffering from a mental disorder is having others around willing to provide social support (Talebi, Matheson, & Anisman, 2016). Younger people with a mental disorder rely heavily on their parents for assistance with dealing with their problem so it is important that parents are educated on what to look for and where to take their child if they suspect a mental illness is at play. This same level of education is also needed within schools so that school counsellors and teachers are able to better recognise and refer students to relevant specialist services (Rickwood, Deane, & Wilson, 2007). Another suggestion to increase the help-seeking motivation of young people is to have General Practitioners conduct lessons around physical and mental health issues, including encouraging students to seek help if they need it, where they can find the help (Rickwood, Deane, & Wilson, 2007). This initiative has been trialled within rural schools and there was a reported decrease in perceived barriers and an increase in help-seeking behaviours (Rickwood, Deane, & Wilson, 2007).
Another strategy that could be implemented is the introduction of a mass media intervention to positively impact expectations, attitudes and intentions of those suffering from a mental disorder (Demyan & Anderson, 2012). Studies in the past have shown that educational campaigns, billboards, and video media have all been effective in increasing intentions and thus increasing the prevalence of help-seeking behaviour (Demyan & Anderson, 2012).
Conclusion
[edit | edit source]Hopefully you can now understand the importance of people seeking help for their mental disorders when they need it and the consequences of not doing so can be tragic. A person's attitude, perception of what others want them to do, familial and social influences, self-efficacy and ideologies all play a pivotal role in determining why one person will be motivated to partake in help-seeking behaviour and others will not. It is important that society as whole continues to educate people on why it is important to seek out help if you need it which will hopefully reduce the stigma surrounding mental illness.
See Also
[edit | edit source]References
[edit | edit source]Barksdale, C. L., & Molock, S. D. (2008). Perceived norms and mental health help seeking among african american college students. Journal of Behavioral Health Services & Research , 36 (3), 285–299. Doi: 10.1007/s11414-008-9138-4
Demyan, A. L., & Anderson, T. (2012). Effects of a brief medial intervention on expectations, attitudes, and intentions of mental health help seeking. Journal of Counseling Psychology , 59 (2), 222–229. Doi: 10.1037/a0026541
Gulliver, A., Griffiths, K. M., & Christensen, H. (2010). Perceived barriers and failitators to mental health help-seeking in young people: A systematic review. BMC Psychiatry , 10 (1), 113–121. Doi: 10.1186/1471-244x/10/113
Levant, R. F., Stefanov, D. G., Rankin, T. J., Halter, M. J., Mellinger, C., & Williams, C. M. (2013). Moderated path analysis of the relationships between masculinity and men's attitudes toward seeking psychological help. Journal of Counselling Psychology , 60 (3), 392–406. Doi: 10.1037/a0033014
Lin, W. B. (2006). A comparative study on the trends of entrepreneurial behaviors of enterprises in different strategies: Application of the social cognition theory. Expert Systems With Applications , 31 (2), 207–220. Doi: 10.1016/j.eswa.2005.09.036
O'Connor, P. J., Martin, B., Weeks, C. S., & Ong, L. (2014). Factors that influence young people's mental health help-seeking behaviour: A study based on the health belief model. Journal of Advanced Nursing , 70 (11), 2577–2587. Doi: 10.1111/jan.12423
Rickwood, D. J., Deane, F. P., & Wilson, C. J. (2007). When and how do young people seek professional help for mental health problems. Medical Journal of Australia , 187 (7), S35–S39.
Rickwood, D., & Thomas, K. (2012). Conceptual measurement framework for help-seeking for mental health problems. Psychology Research and Behavior Management , 5, 173–183. Doi: 10/2147/PREM538707
Roberto, A. J., Shafer, M. S., & Marmo, J. (2014). Predicting substance-abuse treatment providers' communication with clients about medication assisted treatment: A test of the theories of reasoned action and planned behavior. Journal of Substance Abuse Treatment , 47 (5), 307–313. Doi: 10.1016/j/jsat.2014.06.002
Talebi, M., Matheson, K., & Anisman, H. (2016). The stigma of seeking help for mental health issues: Mediating roles of support and coping and the moderating role of symptom profile. Journal of Applied Social Psychology , 46 (8), 470–482. Doi: 10.1111/jasp.12376
Vogel, D. L., Wade, N. G., & Haake, S. (2006). Measuring the self-stigma associated with seeking psychological help. Journal of Counseling Psychology , 53 (3), 325–337. Doi: 10.1037/0022-0167.53.3.325
Wendt, D., & Shafer, K. (2016). Gender and attitudes about mental health help seeking: Results from national data. Health & Social Work , 41 (1), e20–e28. Doi: 10.1093/hsw/hlv089
Whiteford, H. A., Buckingham, W. J., Meredith, G. H., Burgess, P. M., Pirkis, J. E., Barendregt, J. J., et al. (2014). Estimating treatment rates for mental disorders in Australia. Australian Health Review , 38 (1), 80–85. Doi: 10.1071/AH13142
World Health Organisation. (2001, October 4). World Health Report. Retrieved October 19, 2016, from World Health Organisation: http://www.who.int/whr/2001/media_centre/press_release/en/